You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
The immediate replacement of a missing anterior tooth can pose a considerable clinical challenge that necessitates careful consideration of treatment options. Conventionally, implant-supported crowns or fixed dental prostheses are commonly employed for such cases. However, fixed dental prostheses entail the preparation of the adjacent intact teeth, which introduces potential drawbacks.1 Implant-supported prostheses, while effective, may not be universally suitable due to factors such as bone resorption, inadequate bone volume, or patient reluctance to undergo implant surgery due to inconvenience and/or cost.2,3
In scenarios that require an immediate fixed replacement option, the delivery of a fiber-reinforced composite bridge can provide an excellent alternative.4-6These bridges offer a conservative and esthetically pleasing method for replacing missing teeth. By minimizing or eliminating the need for tooth preparation, fiber-reinforced composite bridges not only preserve the integrity of the existing tooth structure but also render the treatment reversible, enabling subsequent restorative changes without causing damage. Furthermore, the fiber-reinforced composite bridge procedure involves chairside fabrication directly in the mouth, which allows it to be accomplished in a single visit, providing a streamlined and efficient solution for immediate anterior tooth replacement.7-9
Clinical Protocol for the Delivery of a Fiber- Reinforced Composite Bridge
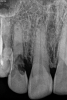
Depending on whether patients present with an existing edentulous space or a non-restorable tooth requiring extraction, as well as other factors, their long-term treatment goals may vary. Nonetheless, each case should be evaluated to identify patients' needs regarding immediate restoration. In the example case presented here, a radiographic examination of a discolored canine lead to the discovery of a lateral incisor (tooth No. 7) with internal resorption that required extraction (Figure 1). The tooth was extracted, and an implant was subsequently placed (Figure 2); however, the patient would be unable to complete the treatment for an extended period of time, so a fiber-reinforced composite bridge was chosen to serve as an ideal long-term provisional replacement option.
1. Isolate the Operating Field
For any adhesive procedure, optimizing bond strength hinges on achieving proper isolation of the operating field. Placing a rubber dam ensures a pristine and fluid-free field, creating an ideal environment for both bonding and the subsequent development of the resin bridge (Figure 3). Achieving complete isolation is particularly important in cases involving replacement of a missing tooth immediately after extraction or implant placement.
2. Precut the Fiber
The fiber-reinforced composite bridge framework design presented here is comprised of a horizontal main fiber spanning the edentulous site to create the bridge scaffold and a vertical reinforcing fiber to support the pontic. The benefit of adding the vertical reinforcing fiber to the bridge framework is that it effectively halts crack development and propagation within the composite under loading conditions. To ensure that the length of the fiber is precise, premeasure the required length in the mouth using a piece of retraction cord. Extending the measuring cord for the horizontal fiber two-thirds of the way across the occlusal surfaces of the abutment teeth will permit sufficient area for bonding and facilitate enhanced fiber stability (Figure 4). Next, place the premeasured cord onto the packaged fiber reinforcement material (Figure 5), mark the length on the package, and cut, leaving the fiber inside the package. Follow this same procedure to cut a smaller portion for the vertical reinforcing fiber. Keep the fibers in their packaging until they are ready for bonding.
3. Prepare the Abutment Teeth
Thoroughly clean the bonding surfaces of the abutment teeth using a mixture of pumice and water to ensure removal of any debris or contaminants. Then, sandblast the bonding surfaces to enhance their surface adhesion and promote a strong bond between the abutment teeth and the bridge materials. After sandblasting, the bonding areas should be etched with a 37% phosphoric acid etchant, taking care to cover the entire surface (Figure 6). This step is crucial for achieving complete bonding of the bridge and preventing potential issues such as leakage and staining over time.
4. Create the Fiber Scaffold
Creation of the fiber scaffold is initiated by bonding the main, horizontal length of fiber reinforcement material to one of the abutment teeth, and then, once stabilized, it is bonded to the other abutment tooth. The fiber reinforcement material should be bonded to the palatal surfaces of the teeth using a bonding agent and a light-cure flowable composite resin. When positioning the fiber reinforcement material on the teeth, it should be kept as incisal as possible to facilitate pontic development while ensuring adequate occlusal clearance. Press the fiber onto the tooth surface, and then, fan it out within the flowable resin (Figure 7). This will increase the surface area to maximize bonding effectiveness. Curve the fiber between the abutment teeth labially to provide space for the reinforcing transverse fiber and the layering composite. Retain the round structure of the fiber in the pontic area for maximum strength.
5. Place the Transverse Vertical Fiber
Using a flowable composite, securely bond the smaller piece of fiber vertically to the palatal aspect of the main fiber, ensuring that it is centered and in proper alignment (Figure 8). Position the vertical fiber such that it will be fully embedded within the planned incisogingival dimension of the pontic. It should not be touching the surface of the tissue at its gingival aspect, and care should be taken to avoid exposure of its incisal aspect during fabrication of the pontic. To maximize the structural integrity of the bridge, ensure a robust connection between the vertical and horizontal pieces of fiber.
6. Begin Developing the Pontic
The most important part of the pontic regarding position, shape, and polish is the surface that will be in contact with the gingiva. An effective way of developing this contour is to employ a sectional matrix band. First, position the matrix band under the vertical fiber reinforcement such that its convex surface is touching the rubber dam (Figure 9). Next, cover the entire fiber assembly with an opaque shade of flowable composite. Direct the composite to flow under the fiber and along the matrix band to develop the desired emergence profile of the pontic. The contact with the band will create a smooth surface that will protect the soft tissue at the site without requiring any further handling (Figure 10 and Figure 11).
7. Complete the Pontic and Finish the Restoration
Continue developing the pontic by layering it with an appropriately selected shade of composite to create an esthetic, well-matched restoration. The degree of layering performed will depend on the esthetic demands of the case and the preferences of the operator. To safeguard the tissues and prevent contamination of the pontic site, the final finishing and shaping of the bridge should be performed before removal of the rubber dam (Figure 12). Any final occlusal adjustments should be performed after rubber dam removal (Figure 13).
Discussion
In the example case presented, the patient returned for evaluation 3 months after implant placement and delivery of the fiber-reinforced composite bridge, and the soft tissue at the site demonstrated adequate growth over the resin pontic (Figure 14). This would provide for a favorable esthetic outcome when the final implant-supported crown was ultimately delivered.
The minimally invasive technique of immediate tooth replacement with a fiber-reinforced composite bridge presents notable benefits when compared with other tooth replacement strategies.6 In addition to being more preservative of the tooth structure than traditional methods, this direct approach facilitates on-the-spot restoration during a single visit, streamlining the process for both patients and dentists. Moreover, the reversibility of treatment with surface-retained bridges offers patients flexibility regarding future treatment options. Fiber-reinforced composite bridges also allow for easy maintenance, reducing the need for complete reconstruction when issues occur in many cases, and they are cost-effective, providing an economically viable solution for patients and ensuring profitability for practices. Their role as a long-term intermediary solution is particularly valuable for patients who have to postpone definitive prosthodontic treatment.6-8
It should be emphasized that the successful delivery of fiber-reinforced composite bridges requires careful case selection and is technique sensitive. Risk factors that may impact the durability of fiber-reinforced composite bridges include the type of material used, the design of the bridge, the oral environment, and the patient's oral hygiene practices.6,9 The affordability of the technique could potentially broaden its use among patients who may not prioritize oral hygiene, and that could result in an increased risk of caries and periodontal diseases. In addition, certain occlusal issues, but particularly limited vertical space, pose a risk of damaging bonded bridges, which have specific interocclusal space parameters.9
Queries regarding this course may be submitted to authorqueries@conexiant.com
About the Author
Saiesha Mistry, BDS, MSc
Accredited Member
American Academy of Cosmetic Dentistry
Associate Fellow
American Academy of Implant Dentistry
Private Practice
Mumbai, India
References
1. Goodacre CJ, Bernal G, Rungcharassaeng K, Kan JY. Clinical complications in fixed prosthodontics. J Prosthet Dent.2003;90(1):31-41.
2. Kermanshah H, Motevasselian F. Immediate tooth replacement using fiber-reinforced composite and natural tooth pontic. Oper Dent.2010;35(2):238-245.
3. Abdullai D, Akdemir O, Cengiz S, Cengiz MI. Single tooth replacement using fiber-reinforced composite resin bridge - a case report. Int J Dent Res.2023;8(3):57-60.
4. Khetarpal A, Talwar S, Verma M. Creating a single-visit, fibre-reinforced, composite resin bridge by using a natural tooth pontic: a viable alternative to a PFM bridge. J Clin Diagn Res.2013;7(4):772-775.
5. Soni M, Sajjanar J, Gade J, et al. Braided glass fiber reinforced composite resin bridge - an alternative treatment for management of missing anterior tooth: a case report. J Pharm Res Int.2021;33(53A):337-342.
6. Vallittu PK, Shinya A, Baraba A, et al. Fiber-reinforced composites in fixed prosthodontics-quo vadis? Dent Mater. 2017;33(8):877-879.
7. Frese C, Schiller P, Staehle HJ, Wolff D. Fiber-reinforced composite fixed dental prostheses in the anterior area: a 4.5-year follow-up. J Prosthet Dent. 2014;112(2):143-149.
8. Martinez ME, Lopez SR, Fontela JV, et al. A new technique for direct fabrication of fiber-reinforced composite bridge: a long-term clinical observation. Dent J (Basel). 2020;8(2):48.
9. Perea-Lowery L, Vallittu PK. Framework design and pontics of fiber-reinforced composite fixed dental prostheses - an overview. J Prosthodont Res. 2018;62(3):281-286.