You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
Dentistry, as a profession, has made major strides when it comes to implant placement proficiency, idealizing the protocols for freehand and guided placement. There are well-established guidelines for proper implant placement. Although proper placement is essential to successful outcomes, the more pertinent and often overlooked challenge faced by the profession is how to properly evaluate the health of implants at routine follow-up appointments. Indeed, there is a dearth of agreement on diagnostic criteria for measuring the long-term health of implants. A need exists for a quantifiable diagnostic tool to expand beyond the current paradigm of simply categorizing implants as a "success" or "failure." Fortunately, new technological advances are being developed to help clinicians in deciphering when the health of an implant is compromised.
Treating Peri-implant Disease
Peri-implantitis affects approximately 5% to 8% of all implants placed.1,2 An array of factors can influence peri-implantitis, and its multifactorial etiology makes treatment complex. Presently, there are no universally agreed upon guidelines or treatment recommendations for treating peri-implantitis once it arises. More research is needed to determine how to properly treat the disease.
Due to the complexity of treating peri-implantitis, there is a need for clinicians to be able to detect peri-implant disease earlier in order to facilitate earlier intervention. If intervention can be rendered earlier, affected implants have a better chance of being salvageable. It should be noted that the successive reimplantation of a dental implant in a site where a previous failure occurred has been associated with a lower success rate.3
Monitoring Implant Health
The primary means by which implant health is monitored include radiographic assessment for bone loss, implant probing to detect bleeding or purulence, and assessment for implant mobility. Although bitewing, periapical, and 3D radiographs can be utilized to visualize implants, their capacity in the diagnosis of peri-implant bone loss may be limited. Due to the density of implants, periapical radiographs do not enable clinicians to visualize the buccal, palatal, or lingual aspects with clarity. Furthermore, cone-beam computed tomography (CBCT) may result in radiation scatter, which can make it difficult to visualize and evaluate peri-implant bone health.
Other methods employed to evaluate the stability of implant sites include dual-energy x-ray absorptiometry (DEXA) scans, simply tapping on the implant, removal torque, and resonance frequency analysis (RFA); however, each of these approaches has limitations. A DEXA scan is impractical for routine dental implant monitoring due to its costly and time-consuming nature and relatively high radiation dose.4 Tapping on an implant has limited clinical value because it is not quantifiable and introduces a high degree of subjectivity. Removal torque involves calculating the amount of force required to remove an implant from its site. Typically, implants with a high removal torque value are more stable. However, removal torque testing can be problematic outside of research settings because it may compromise the bone-to-implant interface.5 RFA, conversely, cannot harm an implant or its surrounding tissue.6 It also provides quantifiable data. However, the implant stability quotient (ISQ) values provided by RFA do not have a universally accepted correlation to stability. Therefore, it requires clinical judgement and interpretation.
Quantitative Percussion Diagnostics
Percussion testing has been utilized in medicine and dentistry for centuries to detect and evaluate organ, joint, and tissue abnormalities.7 Although simple percussion (ie, tapping) is too subjective and limited in diagnostic value to be used to evaluate implant stability, the use of quantitative percussion diagnostics (QPD) to evaluate the health of an implant may provide relevant data regarding structural stability by quantitatively measuring the micromovement created by the percussive force. QPD, which is a noninvasive and nondestructive evaluation method, has existed for almost 20 years but has only recently become available for clinical use. The first QPD device received clearance from the US Food and Drug Administration (FDA) in 2008 to be used in research to measure the micromobility of teeth and dental implants.8
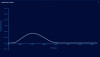
QPD instruments contain a free-floating rod with a force sensor that measures the mechanical response of the implant being percussed (Figure 1). The amount of mechanical energy returned to the rod is then analyzed by software algorithms, which provide critical structural information about the health and stability of the site based on quantifying the amount of overall micromobility of the implant.9 The data is shown as an energy return graph that is ideally shaped like a classic bell curve (Figure 2). The lower the height (ie, amplitude) of a QPD energy return graph, the more mobile the implant and the weaker the osseointegration or bone quality present at the site (Figure 3).9 When QPD is used, a healthy implant and its surrounding bone will exhibit a combination of elastic and anelastic behavior. A healthy implant will dissipate a minimal amount of energy, thus causing the loss coefficient to be greater than zero; however, if the implant is ailing, the loss coefficient will be considerably higher.10 This elevated loss coefficient can alert the clinician that the implant may require intervention and treatment.
In practice, QPD technology may provide critical information related to the implant loading timeline. When an implant is placed, either a single-stage (ie, immediate loading) or two-stage (ie, delayed loading) protocol can be utilized. A delayed loading protocol is often the more conservative option and demonstrates a higher success rate (approximately 96%) when compared with immediate loading.10 In the two-stage approach, the implant is placed and then submerged beneath the soft tissue for several months to permit healing and osseointegration. After the healing period, the implant is uncovered and receives either a provisional or final restoration. In the single-stage approach, the implant is immediately loaded with a provisional or final restoration following placement. The advantage of this approach is that it requires fewer surgeries, may achieve a more esthetic result, and may allow the patient to return to a normal diet sooner; however, research has shown that it has a lower success rate when compared with delayed loading.10,11 Currently, whether or not an implant can be immediately loaded is largely determined by the insertion torque achieved.12 The problem with using insertion torque as the sole determining variable is that it only provides information about an implant's stability at the time of placement. It does not continue to provide information about the implant's stability as it integrates. QPD may be a useful tool in determining whether an implant is sufficiently stable to undergo loading (Figure 4). Furthermore, while an immediately loaded implant is integrating, QPD may, theoretically, enable the clinician to quickly identify if the load on the implant should be removed or if a healing abutment should be replaced.
QPD for Crack Detection in Natural Teeth
Cracks in teeth are particularly difficult to diagnose yet increasingly prevalent. Because patients are living longer, and there is an increasing demand to keep their teeth longer, the prevalence of cracks is on the rise.13 Hilton and Ferracane's work with the National Dental Practice-Based Research Network reported that approximately 66.1% of patients had at least one cracked molar.14 If left untreated, cracked teeth can undergo an insidious progression in which the cracks progress to root fractures and lead to a hopeless prognosis.15
Historically, cracks are detected with magnification, occlusal testing, transillumination, and dye penetrants. The challenge with transillumination is that it may lead to false positives because enamel craze lines that are more superficial in nature can be mistaken for cracks.16 Dye penetrants, such as methylene blue, are commonly utilized to detect cracks. Dye penetrants work because the dye is drawn into cracks through capillary action. However, in many cases, cracks may not be large enough to be able to draw in the dye. And like transillumination, the use of dye also relies on subjective assessment, which may lead to false positives. In effect, when the use of dye penetrants alone are employed for crack detection, it may be misleading.17 By the time that a crack can be detected with the use of a tooth sleuth, the crack may be advanced, and the tooth may have a guarded prognosis. If the tooth elicits pain on release or pressure after occluding, this may indicate that the crack is approximating the pulpal tissue.18 By the time the crack has entered into the pulp complex, the tooth may be beyond repair. The earlier that cracks are detected and managed, the better the prognosis of the tooth.
QPD shows promise in being able to identify localized fractures and cracks in natural tooth structure by detecting their movement within the tooth. In the future, QPD may be helpful in the identification of incomplete fractures in natural teeth as well as failing direct restorations and compromises in the crown-cement interface of indirect restorations; however, FDA clearance has not yet been obtained for these uses (Figure 5). Published studies show that the shape of a QPD energy return graph is created by localized or internal micromovement from small microgap defects.10 The more microgap defects that are present, the more distorted the energy return graph becomes. With the help of another algorithm, the normal fit error, a computer can calculate the severity of the damage by fitting a bell-shaped curve over the energy return graph. The spaces that do not fit within the idealized curve are given a numerical quantification. The greater the normal fit error, the greater the crack severity. This capability to quantify the extent of internal damage may make QPD a promising technology for the early, objective detection of structural compromise that may otherwise be difficult to identify through traditional clinical methods. In fact, in vitro studies have found that QPD technology has been able to detect cracks with 96% specificity and 100% sensitivity.8
Practical Application
Currently, dental team members can utilize QPD to evaluate the stability of implants as it relates to their overall movement measured as micromobility. The less overall mobility in an implant, the more structurally stable the site is. When QPD is used to assess the health of implants after placement and at subsequent examinations and hygiene appointments, it facilitates the development of trend lines that indicate whether the site is becoming healthier or more compromised over time (Figure 6). This permits assessment of whether treatments have been successful or not using quantifiable data.
Conclusion
QPD provides quantifiable information that cannot be "seen" with the current visual technologies that dentistry has depended upon for decades. Due to the mechanical engineering basis of this technology, a clinician can more accurately determine how an implant responds when the patient is eating, bruxing, or clenching. In addition, due to its high sensitivity, the structural breakdown of dental implant sites can be identified earlier when proactive preventive treatment can be most effective.
Hopefully, in the near future, clinicians will also be able to use QPD to evaluate for localized or internal micromobility of an implant or tooth. When these two independent ways of assessing mobility are simultaneously being recorded, clinicians will have even more data on the structural health of their patients' implants and teeth. This technology may be a helpful adjunct to incorporate into all comprehensive exams, routine hygiene visits, and emergency visits. During comprehensive exams, it could provide dentists with vital information about the status of each tooth and implant so that they can generate more thorough treatment plans. And during emergency visits, it could be a helpful resource because the existing methods used to detect incomplete crown fractures and failing restorations are not conclusive.
Queries regarding this course may be submitted to authorqueries@conexiant.com
Melissa Seibert, DMD, MS
Diplomate
American Board of General Dentistry
Creator and Host
Dental Digest Podcast
Founder
Elevated.GP
Clinical Instructor
Creighton University School of Dentistry
Omaha, Nebraska
Private Practice
Richmond, Virginia
References
1. Atieh MA, Alsabeeha NHM. Peri-implantitis through the looking glass. Int Dent J. 2024;74(1):42-45.
2. Berglundh T, Persson L, Klinge B. A systematic review of the incidence of biological and technical complications in implant dentistry reported in prospective longitudinal studies of at least 5 years. J Clin Periodontol.2002;29(Suppl 3):197-212.
3. Agari K, Le B. Successive reimplantation of dental implants into sites of previous failure. J Oral Maxillofac Surg.2020;78(3):375-385.
4. Devlin H, Horner K, Ledgerton D. A comparison of maxillary and mandibular bone mineral densities. J Prosthet Dent.1998;79(3):323-327.
5. Kim H-J, Park H-S. Long-term evaluation of factors affecting removal torque of microimplants. Prog Orthod. 2021;22(1):42.
6. Yamaguchi M, Xu H, Shimizu Y, et al. Resonance frequency analysis of long-term implant success in the posterior partially edentulous mandible. Quintessence Int.2008;39(3):e121-e125.
7. Stanford Medicine. The birth of percussion. Stanford Medicine 25 website. https://stanfordmedicine25.stanford.edu/blog/archive/2014/The-Birth-of-Percussion.html. Published October 23, 2014. Accessed June 5, 2025.
8. Sheets C. Quantitative percussion diagnostics: going beyond the human eye. Spear Education website. https://www.
speareducation.com/spear-review/2025/02/quantitative-
percussion-diagnostics-going-beyond-the-human-eye. Published February 25, 2025. Accessed June 5, 2025.
9. Amiri M, Crawford GA, Earthman JC. Quantitative percussion diagnostics for evaluating porosity and surface roughness of cold sprayed and laser deposited materials. J Mater Res Technol. 2021;14:312-323.
10. VanSchoiack LR, Shubayev VI, Myers RR, et al. In vivo evaluation of quantitative percussion diagnostics for determining implant stability. Int J Oral Maxillofac Implants. 2013;28(5):1286-1292.
11. Zembić A, Glauser R, Khraisat A, Hämmerle CH. Immediate vs. early loading of dental implants: 3-year results of a randomized controlled clinical trial. Clin Oral Implants Res. 2010;21(5):481-489.
12. Lang NP, Lindhe J, Sanz M, Chapple ILC, eds. Lindhe's Clinical Periodontology and Implant Dentistry. 7th ed. Wiley-Blackwell; 2021.
13. Sheets CG, Stewart DL, Wu JC, Earthman JC. An in vitro comparison of quantitative percussion diagnostics with a standard technique for determining the presence of cracks in natural teeth. J Prosthet Dent.2014;112(2):267-275.
14. Hilton T, Ferracane J. Cracked teeth registry. Kaiser Permanente Center for Health Research website. https://www.kpchr.org/ndpbrn/public/pages/meetings/assets/2013-
AnnMtg/Cracked_Teeth_Registry-Tom_Hilton-Jack_Ferracane.pdf. Published September 28, 2013. Accessed June 5, 2025.
15. Krishnan U, Moule A, Michael S, Swain M. Fractographic analysis of a split tooth presenting radiographically as a horizontal root fracture in an unrestored mandibular second molar. J Endod. 2018;44(2):304-311.
16. Rubinstein R. The anatomy of the surgical operating microscope and operating positions. Dent Clin North Am.1997;41(3):391-413.
17. Wright HM Jr, Loushine RJ, Weller RN, et al. Identification of resected root-end dentinal cracks: a comparative study of transillumination and dyes. J Endod. 2004;30(10):712-715.
18. Kahler W. The cracked tooth conundrum: terminology, classification, diagnosis, and management. Am J Dent.2008;21(5):275-282.