You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
Conventional heat-polymerized polymethyl methacrylate (PMMA) dentures have demonstrated decades of predictable clinical performance, with reported fracture rates ranging from 3% to 10% annually, depending on arch configuration, opposing dentition, and parafunctional activity.1-3 The first year following delivery has historically represented the highest period of adjustment and complication, reflecting occlusal equilibration and residual ridge remodeling.
Innovative manufacturing modalities have introduced additive manufacturing via digital scanning, computer-aided designed (CAD), milling, and 3D printing as viable alternatives to traditional analog workflows. Although these technologies improve reproducibility and efficiency, early-generation printable denture resins demonstrated reduced fracture toughness compared with heat-processed PMMA.4-6 Contemporary high-impact printable PMMA-based resins incorporate enhanced cross-linking chemistry and optimized post-curing protocols, and laboratory studies report improved flexural and impact strength.7-10 Nevertheless, clinical survival reflects not only polymer properties but also digital design accuracy, occlusal planning, reinforcement strategy, and work-flow adherence.
Additive denture fabrication introduces unique variables that influence structural durability. These variables include scan fidelity and tissue capture accuracy, CAD-controlled base thickness, precision of occlusal simulation, print orientation, resin storage and preparation, and post-curing consistency, and whether fabrication occurs in centralized laboratory environments or chairside settings. Understanding the interplay of these factors is essential for achieving predictable outcomes.
Recognizing those shortcomings, manufacturers have developed high-impact resins specifically engineered for denture base 3D printing applications. Lucitone Digital Print Denture System (LDP) (Dentsply Sirona, Charlotte, North Carolina) and SprintRay High Impact Denture (SRHI) (SprintRay, Los Angeles, California) represent two of the most widely adopted resins in this category. Both promise enhanced fracture resistance, improved impact tolerance, and clinical reliability. However, much of the evidence supporting these claims has been limited to in vitro testing or small-scale clinical studies.7-9
Overview of High-Impact Printable Resins
Modern printable denture base materials are photopolymerized PMMA-based resins engineered to improve impact resistance and fracture toughness relative to earlier printed formulations.4-9 Mechanical improvements over first-generation materials include increased cross-link density, improved polymer homogeneity, optimized post-polymerization curing protocols, hardware improvements introduced in the past 2 years, and reduced internal porosity.11
Despite these advancements, material properties alone do not determine clinical success. Centralized laboratory workflows may provide more consistent printing processes as well as post-curing and quality controls, whereas chairside fabrication requires meticulous adherence to protocol to minimize variability. Clinical outcomes therefore reflect the interaction between intrinsic material strength and execution of established prosthodontic principles.
Study Design and Methods
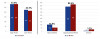
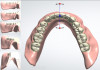
Between January and June 2023, 1,011 dentures were fabricated and inserted across multiple clinical sites in the United States. Both maxillary (53.8%) and mandibular (46.2%) prostheses were included, and the majority opposed another prosthesis (80.4%), with a smaller percentage opposing natural dentition (15.9%) as illustrated in Figure 1.
Inclusion criteria consisted of definitive and immediate complete dentures fabricated with high-impact printable materials that were inserted and functionally delivered. Interim appliances intended for short-term use and prostheses not inserted intraorally were excluded from survival analysis.
Survival was defined as continued intraoral function without catastrophic structural failure requiring replacement. Failure was defined as structural fracture or irreparable compromise necessitating remake. Catastrophic fracture was defined as loss of structural integrity rendering the prosthesis non-serviceable.
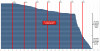
Planned transitions from immediate to definitive dentures were censored from survival calculations to avoid misclassification of transitional therapy as mechanical failure, as demonstrated in Figure 2. Mean time to failure was calculated from insertion to discontinuation, and fracture patterns were analyzed longitudinally (Figure 3). Statistical comparisons were conducted with significance defined at p < 0.05, and confidence intervals were evaluated when appropriate.
Potential sources of bias included the non-randomized study design, variability in clinician experience, mixed centralized and chairside fabrication environments, and unequal distribution of immediate dentures between cohorts, which may affect the validity of the root cause analysis (RCA) conclusions.
Clinical Survival Patterns
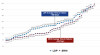
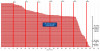
Overall cumulative fracture reached 9.5% at 18 months, representing 96 fractures among 1,011 dentures (Figure 4). Fracture incidence increased progressively during the first year and plateaued thereafter, suggesting that early mechanical or design-related issues were the primary determinants of long-term performance.
Immediate dentures demonstrated higher early discontinuation rates, largely attributable to ridge remodeling and transitional treatment sequencing rather than intrinsic structural weakness (Figure 5). When immediate dentures were censored from survival analysis, definitive prostheses demonstrated stable survival patterns across work-flows.
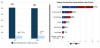
Root cause analysis revealed that more than half of fractures were attributable to design-related deficiencies (Figure 6). These deficiencies most frequently included insufficient denture base thickness, midline stress concentration, inadequate reinforcement, and occlusal imbalance. Material-related compromise accounted for approximately 17% of fractures, while work-flow related variables such as scan inaccuracy or fabrication deviations represented approximately 7% of failures.
New denture designs demonstrated a higher fracture incidence compared with reprints derived from validated digital files (Figure 7 and Figure 8), suggesting that iterative design refinement improves structural predictability.
Root Cause Analysis
The distribution of fracture etiology reinforces a fundamental prosthodontic principle: material strength cannot compensate for compromised biomechanical design. When base thickness is insufficient or occlusal forces are poorly distributed, tensile stress concentrates in high-risk regions regardless of polymer chemistry. Design deficiencies were therefore the dominant contributor to structural failure, while material compromise represented a minority of cases (Figure 9 and Figure 10).
Immediate Versus Definitive Dentures
Immediate dentures inherently experience rapid residual ridge resorption, soft tissue remodeling, and occlusal instability during early healing phases. These biological changes alter stress distribution and increase the likelihood of fracture independent of material properties. For this reason, immediate prostheses must be analyzed separately from definitive appliances when interpreting survival data. Once transitional factors are removed from analysis, definitive prostheses demonstrate survival trends comparable to conventional PMMA expectations9,12 (Figure 11).
Clinical Design Recommendations
Minimum base thickness should be maintained between 2.5 millimeters and 3.5 millimeters in stress-bearing regions, particularly across the mandibular midline (Figure 12 and Figure 13). In cases presenting with thin mandibular ridges or parafunctional activity, reinforcement strategies such as fiber incorporation or metal framework support should be considered to enhance structural resistance.
Occlusal design should incorporate digitally simulated bilateral balance and minimize cantilevered force vectors to reduce tensile concentration within the denture base. Scan verification protocols should confirm accurate border extension, precise intaglio adaptation, complete tissue capture, and validated occlusal simulation prior to fabrication.
A reprint of a prior digital design may be appropriate when the structural framework remains sound and failure is attributable to isolated processing defects. Conversely, a remake is indicated when structural design deficiencies, such as inadequate thickness or occlusal imbalance, are identified as the primary cause of fracture. Therefore, the remake incorporates a better fit to the underlying ridge.
Risk Factors for Early Printed Denture Failure
Early fracture patterns in this cohort demonstrated a clear clustering within the first year of service, indicating that initial biomechanical adaptation and digital execution play a critical role in long-term durability. Multiple clinical and technical variables were identified as increasing susceptibility to early structural compromise.
Immediate denture delivery represents one of the most significant risk factors. Following extraction, rapid residual ridge resorption and soft tissue remodeling alter the intaglio surface relationship and occlusal scheme. As adaptation changes, uneven load distribution may develop across the denture base (Figure 14). These transitional stresses increase flexural strain, particularly across the mandibular midline, and may predispose the prosthesis to fracture independent of resin chemistry. For this reason, immediate dentures inherently demonstrate higher early discontinuation rates and must be interpreted separately from definitive prostheses.
Thin mandibular denture bases also represent a primary structural vulnerability. The mandibular arch is biomechanically predisposed to flexure during function due to muscular attachments and arch configuration. When base thickness is reduced below recommended parameters, particularly across the lingual flange and midline, tensile forces concentrate and microfracture propagation may occur. Even minor reductions in thickness can significantly increase flexural stress under masticatory load.
Opposition by natural dentition further elevates fracture risk. Natural teeth generate greater occlusal force magnitude and more localized contact points compared with opposing complete dentures. When printed dentures oppose natural dentition, stress distribution becomes less uniform, increasing the likelihood of crack initiation at high-load zones.
Parafunctional activity, including bruxism and clenching, introduces repetitive cyclic loading that exceeds typical masticatory patterns. Repetitive tensile stress accelerates fatigue failure, particularly in areas of reduced thickness or structural irregularity. In such patients, reinforcement strategies and occlusal adjustments become increasingly important.
Poor scan fidelity represents a digital risk factor unique to additive workflows. Inaccurate border capture, incomplete tissue registration, or surface distortion may result in improper adaptation and instability. Instability during function increases localized loading and may compromise long-term structural integrity. Unlike analog impressions, digital inaccuracies may be subtle and require deliberate verification prior to print approval.
Occlusal imbalance and inadequate digital articulation simulation further contribute to early fracture risk. Failure to simulate bilateral balanced occlusion or to eliminate cantilevered force vectors results in concentrated stress zones within the denture base. When these stresses coincide with thin sections or structural transitions, fracture risk increases substantially.
Additional contributing factors may include insufficient post-curing protocols, print orientation that produces unfavorable layer stress alignment, and limited experience with digital design software. Each of these variables emphasizes that additive denture success depends on strict adherence to both prosthodontic fundamentals and digital work-flow discipline.
Collectively, these risk factors underscore that early printed denture failure is multifactorial. Material properties play a role, but the interaction between biological remodeling, biomechanical design, and work-flow execution exerts a far greater influence on early structural durability.
Limitations
Several limitations must be considered when interpreting the findings of this multicenter evaluation. The follow-up period was limited to approximately 21 months, which restricts conclusions regarding long-term survival beyond the early and mid-term phases. Conventional PMMA dentures often demonstrate fracture trends over extended periods, and comparable longitudinal data for printable resins will require multi-year observation.
The study design was prospective but non-randomized, introducing potential selection bias. Denture type distribution, including the proportion of immediate versus definitive prostheses, varied across fabrication pathways. Although transitional appliances were censored from survival calculations when appropriate, unequal case distribution may still influence subgroup interpretation.
Variability in clinician experience and digital workflow proficiency represents another potential confounding factor. Additive denture fabrication involves multiple operator-dependent steps, including scanning, CAD modification, print orientation selection, resin storage and preparation post-processing, and finishing. Differences in training and adherence to protocol across sites may influence fracture incidence independent of material characteristics.
The study incorporated both centralized laboratory fabrication and chairside production. While this reflects real-world clinical practice, the heterogeneity of equipment, curing protocols, and quality control measures introduces variability that cannot be completely standardized.
Root cause analysis relied on clinical assessment of fracture etiology, which may involve subjective interpretation when categorizing failures as design-related, material-related, or work-flow related. Although structured criteria were applied, overlap between categories is possible in multifactorial fracture events.
Additionally, opposing dentition type, parafunctional habits, ridge morphology, and patient-specific functional patterns were not fully stratified in a controlled manner. These patient-related variables can significantly influence mechanical loading and survival outcomes.
Finally, because the evaluation focused on high-impact printable PMMA-based resins, findings may not be directly generalizable to all printable denture materials currently available or to future generations of polymer systems with different mechanical properties.
Despite these limitations, the data provide valuable insight into survival patterns and fracture etiology under routine clinical conditions. The findings support a design-centered framework for additive denture fabrication while highlighting areas requiring continued longitudinal investigation.
Clinical Takeaways
Successful integration of additive denture fabrication into clinical practice depends less on the specific printable resin selected and more on adherence to fundamental biomechanical and digital design principles. The present analysis demonstrates that most structural failures are attributable to design execution rather than intrinsic material compromise, underscoring the continued relevance of traditional prosthodontic fundamentals within digital workflows.
Base thickness remains a primary determinant of fracture resistance. Clinicians should ensure a minimum base thickness of 2.5 millimeters to 3.5 millimeters in stress-bearing regions, particularly across the mandibular midline, where tensile forces commonly concentrate. In cases involving thin residual ridges, high muscle attachment, or opposing natural dentition, additional reinforcement through fiber integration or metal substructure should be considered to reduce midline flexure.
Occlusal scheme design is equally critical. Digitally simulated bilateral balanced occlusion should be verified prior to final print approval. Premature contacts, cantilevered force vectors, or uneven posterior load distribution increase localized stress concentration and elevate fracture risk. Attention to occlusal harmony remains essential regardless of fabrication method.
Scan fidelity and digital verification protocols should not be overlooked. Border extension accuracy, intaglio surface adaptation, and tissue capture completeness must be confirmed before fabrication. Inaccurate scanning or incomplete capture can lead to poor adaptation, instability, and subsequent structural compromise.
Immediate dentures require separate clinical interpretation from definitive prostheses. Early fracture or discontinuation in immediate appliances frequently reflects post-extraction ridge remodeling and occlusal instability rather than failure of the printable material. For this reason, immediate dentures should be excluded from definitive survival comparisons when assessing long-term outcomes.
Reprint versus remake decisions should be guided by structural analysis. When the underlying digital design remains biomechanically sound and failure is attributable to isolated fabrication error, a reprint may be appropriate. However, when fracture originates from inadequate thickness, occlusal imbalance, or reinforcement deficiency, a remake with corrected design parameters is indicated.
Finally, clinicians should recognize specific risk factors that predispose to early printed denture failure. These include immediate denture delivery, thin mandibular bases, opposition by natural dentition, parafunctional activity, poor scan accuracy, and unbalanced occlusion. Identifying these variables during treatment planning allows proactive modification of design to improve longevity.
Summary
This prospective multicenter analysis reinforces that the clinical performance of high-impact 3D-printed dentures is governed primarily by biomechanical design integrity and work-flow precision rather than resin chemistry alone (Figure 15). Although contemporary printable materials demonstrate improved mechanical properties compared with earlier formulations, structural success depends on adequate base thickness, reinforcement planning, occlusal balance, and accurate digital capture.
Fracture incidence in this cohort reached 9.5% at 18 months, with most failures occurring during the first year and stabilizing thereafter. This early clustering parallels historical adaptation trends observed in conventional PMMA dentures and highlights the importance of the initial adjustment period. Once prostheses remain intact beyond this early phase, mid-term survival appears favorable.
Root cause analysis demonstrated that design-related deficiencies accounted for the majority of fractures, while material-related compromise represented a minority of cases. Workflow related variables, including scan fidelity and post-processing consistency, also contributed but were secondary to biomechanical planning. Immediate dentures exhibited higher early discontinuation rates due to biological remodeling and transitional therapy, emphasizing the need to interpret survival data within the context of intended prosthesis service life.
From a clinical perspective, the findings support a risk-based framework for additive denture fabrication. Identifying patient-specific and design-specific risk factors allows targeted reinforcement, occlusal modification, and thickness control before fabrication. When digital workflows are executed with the same biomechanical rigor traditionally applied to conventional dentures, additive prostheses can achieve predictable short- to mid-term clinical performance.
Ultimately, the transition to digital removable prosthodontics should not be viewed as a material-driven evolution but as a design-driven discipline. The durability of printed dentures is determined less by the brand of resin used and more by how carefully prosthodontic principles are integrated into digital planning and fabrication protocols.
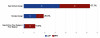
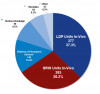
This study demonstrates the clinical viability of high-impact 3D-printed denture resins, with both LDP and SRHI performing comparably to conventional PMMA under real-world conditions. The two materials had similar fracture rates, with no significant difference between LDP (47%) and SRHI (49%). Mean time to breakage was also similar, with a difference of 36 days between groups. Some SRHI breakages could account for immediate dentures post-extractions, which could also have led to the shorter mean average time to breakage. These findings are clinically significant, as they provide practitioners with real-world data supporting the shift toward digital prosthodontics and additive manufacturing technologies13-16 (Figure 16 and Figure 17). It is important to note that there has been advancements in the materials with the introduction of SprintRay’s next generation material now known as Apex with improved performance and translucency.
Acknowledgement: The authors would like to thank Frank Linder for creation of Figure 12 to Figure 14.
Eric D. Kukucka, DD
Aspen Dental,
Chicago, Illinois
Sundeep Rawal, DMD
Aspen Dental,
Chicago, Illinois
Nassif Youssef, BDS, CAGS
Aspen Dental,
Chicago, Illinois
Arwinder Judge, DDS
Aspen Dental,
Chicago, Illinois
Joshua Dartez
Aspen Dental,
Chicago, Illinois
Gregori M. Kurtzman, DDS
Private practice,
Silver Spring, Maryland
References
1. Bamakan SMH, et al. Evaluation of the mechanical properties of high-impact acrylic denture base materials. J Prosthodont. 2017;26:528-535.
2. Peixoto LAP, et al. Fracture toughness and impact strength of heat-cured and cold-cured denture base resins. J Prosthodont. 2014;23:41-47.
3. Santos MD, et al. Mechanical performance of denture base resins: comparative study between cold-curing and heat-curing materials. J Prosthet Dent. 2017;117:630-636.
4. Altarazi A, Haider J, Alhotan A, Silikas N, Devlin H. Current progress in the development of resin materials with nanofillers for 3D printing of denture base. Prosthesis. 2024;6:770-797.
5. Majeed HF, Hamad TI, Bairam LR. Enhancing 3D-printed denture base resins: a review of material innovations. Sci Prog. 2024;107:368504241263484.
6. Li P, Lambart AL, Stawarczyk B, Reymus M, Spintzyk S. Postpolymerization of a 3D-printed denture base polymer: impact of post-curing methods on surface characteristics, flexural strength, and cytotoxicity. J Dent. 2021;115:103856.
7. Prakash J, Shenoy M, Alhasmi A, Al Saleh AA, C SG, Shivakumar S. Biocompatibility of 3D-printed dental resins: a systematic review. Cureus. 2024;16(1):e51721.
8. Mosaddad SA, Khorasani E, Schimmel M, et al. Do resin-modified 3D-printed complete dentures show improved mechanical, physical, surface, and biological properties? A systematic review and meta-analysis. J Dent. 2025;161:105983.
9. Mann RS, Ruse ND. Fracture toughness of conventional, milled, and 3D-printed denture bases. Dent Mater. 2022;38:1443-1451.
10. Al-Dwairi ZN, et al. Mechanical properties of 3D-printed denture base resins: a systematic review. J Prosthet Dent. 2022;128:1031-1039.
11. Duangsuwan J, Kantikosum K, Fan Y, Giordano R. Accuracy evaluation of different denture bases fabricated by 3D-printing technology. Presented at: International Association for Dental Research/American Association for Dental Research/CANADIAN Association for Dental Research General Session; 2020.
12. Zarb GA, Fenton AH, et al, eds. Prosthodontic Treatment for Edentulous Patients: Complete Dentures and Implant-Supported Prostheses. 13th ed. St Louis, MO: Elsevier Mosby; 2013.
13. Phoenix RD, Engelmeier RL. Laboratory and clinical performance of heat-polymerized PMMA denture bases. J Prosthet Dent. 1997;78:177-182.
14. Goodacre CJ, et al. Digital prosthodontics: a review of current technologies and future directions. J Prosthet Dent. 2020;124:680-686.
15. Smets K, Vandeweghe S, Ongenae L, D’haese R. Complications of 3D-printed dentures: a systematic review. J Prosthet Dent. 2025;S0022-3913(XX)00455-X. (Needs volume/pages once finalized — likely in press/online ahead of print)
16. Anadioti E, Musharbash L, Blatz MB, Papavasiliou G, Kamposiora P. 3D-printed complete removable dental prostheses: a narrative review. BMC Oral Health. 2020;20:343.