You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
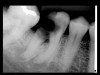
The decision to retain or extract a questionable tooth is one that occurs frequently in dental practice. There are many factors to consider when making this decision. Some situations are very straightforward (Figure 1) while others fall into a “gray” area of decision-making (Figure 2). This article will provide guidelines for determining whether to extract or retain a tooth when the decision is not so straightforward using structural, periodontal, endodontic, and esthetic criteria. Some teeth may involve only one of these areas, and some will involve various combinations of these areas. There are also other important factors to consider such as patient expectations, patient finances, and patient compliance, but these topics vary from patient to patient and should be discussed with each individual patient. While these topics are very important to the decision-making process, they are beyond the scope of this article.
Structural Parameters
Teeth that have either fractured or have decay at or near the crestal bone fall into a gray area for decision-making. The questions become, “How much tooth structure is needed to obtain a predictable result?” and “What are the options for obtaining tooth structure if enough structure is not present?” To answer these questions, two pieces of information are required. First, how much ferrule is necessary to obtain a predictable result? Second, what is the patient’s biologic width? Starting with the first question, ferrule is defined as “the amount of tooth structure between the margin of the restoration and the margin of the build-up.”1 As derived from bench-top laboratory studies, the minimum vertical distance of remaining tooth structure required for a bonded restoration is 1.5 mm on the facial and lingual of the tooth to prevent fatigue resistance,2 and the minimum horizontal thickness of remaining tooth structure is 1 mm.3 Keeping within these limits will ensure the adequate resistance form necessary to prevent dislodgment of the restoration.
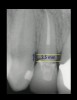
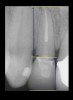
If the tooth has been endodontically treated, the remaining tooth structure relative to the post space needs to be evaluated. The Rule of Thirds is used in this situation. It states that the canal or canal space preparation should not be any wider than one third the mesiodistal root diameter after the endodontic access (Figure 3).3 Once the clinician determines whether adequate tooth structure is present, the second area to evaluate is the distance of the fracture/caries from the crest of bone. To avoid biological width impingement, the minimum distance needed from the osseous crest to the final margin placement is 2.5 mm (Figure 4). As determined in cadaver studies, this consists of approximately 1 mm of connective tissue attachment, 1 mm of junctional epithelium, and 0.5 mm of gingival sulcus.4 This measurement is meant as a guideline and not an absolute number, as it has been shown to have individual variability.5 This actual dimension for the individual patient can be predictably determined by sounding to bone on the adjacent teeth to more closely determine the individual’s biologic width.6
The clinical guideline of 4 mm—consisting of 1.5 mm of tooth structure and 2.5 mm biologic width1,3—is, therefore, the minimum limit for tooth structure above the alveolar bone (Figure 5). If this parameter cannot be met, there are two options for obtaining this threshold. One option is surgical crown lengthening,7,8 and the other is forced orthodontic eruption.9 The choice between each option should be made based on the effect each procedure will have on the esthetics of the case, the crown-to-root ratio, and whether osseous surgery will create a furcation involvement on the adjacent teeth (Figure 6). Esthetic considerations will be addressed later. In terms of crown-to-root ratio, there are two guidelines that exist for determining the minimum ratio (Figure 7). One is the classical 1:1 presented by Penny.10 The second, for maxillary anterior teeth, is 12 mm to 13 mm of tooth with 8 mm to 9 mm of root in bone and 4 mm coronal to the bone, as presented by Spear.1 If all of these criteria for tooth structure are met, then the tooth should be considered an acceptable candidate for retention and restoration. Also, if insufficient tooth structure exists, the required tooth structure can be obtained via forced orthodontic eruption or periodontal surgery provided that the esthetics and periodontal function of the tooth in question and the adjacent dentition are not compromised.
Periodontal Parameters
Periodontal disease is prevalent in the adult population. The severity of periodontal disease and whether it is generalized or localized will play a role in the decision of whether to restore or extract the affected tooth. The areas of concern are pocket depth; bone loss; bone defect morphology; furcation involvement; and host susceptibility.
Measurement of the pocket depth is one method for determining the severity of periodontal disease. Pocket depth is defined as the distance from the free gingival margin to the base of the sulcus. With the exceptions of gingival overgrowth and pseudo-pockets, deep probing depths (> 4 mm) with bleeding are an indicator of active periodontal disease and future attachment loss. Although pocket depth may change over time as a result of changes in the position of the free gingival margin, studies indicate that a pocket depth of 5 mm or greater is a indication of past periodontal disease.11 Deeper pocket depths (> 7 mm) also have been shown to be more difficult to maintain over time.12-14 Therefore, pocket depths over 7 mm should have a greater consideration for extraction than pocket depths of < 5 mm with all other factors being equal. These parameters are based on longitudinal research.
Bone loss is an indicator of past periodontal disease as well. Gustavo et al have established a guideline for percentage of bone loss relative to long-term prognosis.15 Bone loss percentage calculation was based on the total length of the root from the cemento-enamel junction to the apex minus approximately 2 mm (biologic width) to the length of the root supporting the alveolar bone. They divided bone loss into three categories < 30% (predictable),16,17 30% to 65% yellow (caution),18-20 and > 65% (consider extraction).13 This does not mean that all teeth with greater than 65% of bone loss need to be extracted; rather, teeth in this category as a whole have a poorer prognosis than teeth with less than 65% bone loss.
Bone defect morphology plays an important role in the predictability of tooth retention as well. Horizontal defects are unpredictable to guided tissue regeneration attempts (Figure 8). Narrow vertical defects respond more favorably to regeneration attempts (Figure 9).21
Furcation involvement also needs to be evaluated. Furcation involvement is classically divided into three categories. Class I furcation involvement is assigned when the furcation is < 3 mm of horizontal penetration. Class II is > 3 mm but is not through and through. Class III has a through-and-through probing.22 Class I defects can be treated and maintained predictably.23,24 Class II defects can be treated successfully25,26 (Figure 10) but long-term maintenance can be a concern.27 Class III defects have been shown to have a poor long-term prognosis (Figure 11).28,29 These recommendations are based on a review of the literature. Host susceptibility is a multi-factorial topic that includes smoking and systemic conditions. Smoking is a major risk factor to periodontal disease progression; it has been shown to have an influence on the odds of developing periodontal disease,30 the impairment of polymorphonuclear cells, reduced immunoglobulins, and compromised wound-healing abilities.31,32 All of these factors together make retaining teeth with a questionable prognosis more challenging.
Diabetes is a systemic condition that affects the periodontium. It has some of the same disadvantages as smoking. Impaired neutrophil function, excessive inflammatory response, collagen turnover defects, and impaired wound healing all are consequences of uncontrolled diabetes.33 The key for the clinician is to determine the control the patient has on the disease process. An uncontrolled patient will make retaining questionable teeth much more challenging than a patient who is controlled through diet and/or medication.
Endodontic Parameters
There has been much discussion recently about the success rates of implants versus the success rates of endodontic therapy. Assuming the tooth is structurally restorable, two questions must be answered to determine whether tooth retention or extraction is needed. First, what are the existing conditions that will affect the long-term prognosis of the chosen therapy? Second, what are the success rates of initial therapy, retreatment, initial apical surgery, and subsequent apical surgery?
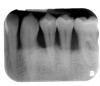
A tooth that is deemed structurally restorable and periodontally sound that requires endodontic therapy has an overall success rate of 90%. There are certain conditions that lower the success rate of which the clinician needs to be aware. According to the Toronto Study,34 a longitudinal study, a vital tooth requiring initial therapy will have a success rate of 93%. A non-vital tooth with a periapical radiolucency < 5 mm will have a 89% success rate.34 A non-vital tooth with periapical radiolucency > 5 mm will have a 74% success rate.34 Clearly, a tooth with periapical radiolucency > 5 mm significantly decreases the success rate of endodontic therapy (Figure 12).
What if the tooth has had previous endodontic therapy? What are the success rates of surgical versus non-surgical therapy and do they change over time? Success rates for surgical re-treatments were found to be higher (77.8%) at 2 to 4 years compared to non-surgical treatment (70.9%).34 However, at 4 to 6 years, non-surgical re-treatment showed a success rate of 83% while surgical re-treatment showed a success rate of 71.8%.34 There was a further decline at > 6 years to 62.9% in the surgical re-treatments.34 There were no papers available that evaluated non-surgical re-treatments after 6 years.35 It appears that if choosing between surgical versus non-surgical therapies to retain teeth, endodontic surgery offers more favorable initial success, but non-surgical retreatment offers a more favorable long-term outcome based on this review of the literature (Figure 13).
Esthetic Parameters
The esthetic parameters will be largely defined on how removal or retention of the tooth will affect the underlying bone and soft-tissue drape. There are two critical questions to consider. First, if the tooth is retained and surgery is necessary, will an esthetic result be possible? And second, if the tooth is removed, will the subsequent bone loss affect the soft-tissue drape negatively? This section will outline what is considered esthetic in the anterior portion of the dentition and will assume that deviation from this is considered “unesthetic.”
Tooth Proportions
Will the retention or removal of the tooth allow tooth proportions to be in the 75% to 86%36 height-to-width ratio? If the answer is yes, then proceed. If the answer is no, then orthodontic or periodontal procedures or both will need to be performed to place the tooth or the osseous crest in the correct esthetic position (Figure 15');" rel="imagepop" rem="#ip:figure14 and Figure 15">Figure 14 and Figure 15).
Gingival Margin Location/Symmetry
Will the removal or retention of the tooth allow gingival symmetry? Gingival symmetry is defined as an imaginary line that should be collinear, connecting the central incisors and canines and parallel with the interpupillary line or horizon if the interpupillary line is canted. Ideally, this line should also be parallel to the incisal edge and the curvature of the lower lip.37 The gingival margin of the lateral incisor should be even with or coronal to this line by a maximum of 3 mm (Figure 16).38 If these parameters are not met, then orthodontic or periodontal procedures or both will need to be performed to place the tooth in the correct esthetic position.
Papilla
Kockich et al studied esthetic papilla asymmetry in bilateral and unilateral situations.37 The results showed that orthodontists rated a unilateral papillary height discrepancy unattractive when it was 0.5 mm to 1 mm more coronal than the adjacent papillae. General dentists rated a 0.5-mm decrease in papillary height as unattractive (Figure 18');" rel="imagepop" rem="#ip:figure17 and Figure 18">Figure 17 and Figure 18). In contrast, the layperson group did not perceive a significant difference in attractiveness even when evaluating the maximum 2-mm deviation in papillary height given in the study.
Bilateral papillary asymmetry results showed the orthodontic group rating a 1-mm uniform reduction in papillary height from canine to canine as less attractive than the ideal smile with normal papillary heights. The layperson group required a decrease in papillary height of 1.5 mm before they rated it as significantly less attractive. The dentists could not detect a significant decrease in papillary height even when uniformly reduced by 2 mm.
The results of this study give the clinician some relative guidelines. Papillary heights must be evaluated both bilaterally and unilaterally. If retention or extraction of a tooth will cause a change in symmetry unilaterally of more than 2 mm, it will be regarded as unattractive. In a bilateral situation, the general public finds a discrepancy of more than 1.5 mm to be unattractive but the general dentist did not see the discrepancy as unattractive even at 2 mm. In cases where papilla heights will be uniformly short, the clinician should be aware that what they see as attractive—a discrepancy of 2 mm—the patient might view as unattractive because they have a smaller tolerance for the discrepancy.
Conclusion
There are many factors to consider when determining whether to retain or to remove and replace a tooth with a prosthesis better serves the patient. The clinician must always remember to present options and probable success rates to help the patient conclude what is best for them. The guidelines discussed in this article will give the clinician a starting point in each of the major clinical categories: structural, periodontal, endodontic, and esthetic. From these parameters the clinician will be able to determine if the tooth is too high a risk for retention. From there, a treatment plan can be created for the patient that incorporates treatment modalities that will increase the chances for long-term success for the future prosthesis.
References
1. Spear FM. Restorative considerations in deciding whether to restore or remove endodontically treated teeth. Advanced Esthetics & Interdisciplinary Dentistry. 2007;3(1):2-10.
2. Ma PS, Nicholls JI, Junge T, et al. Load fatigue of teeth with different ferrule lengths, restored with fiber posts, composite resin cores, and all-ceramic crowns. J Prosthet Dent. 2009;102(4):229-234.
3. West JD. Endodontic predictability—Restore or Remove: How do I choose? In: Cohen M, ed. Interdisciplinary Treatment Planning: Principles, Design, Implementation. 1st ed. Hanover Park, IL: Quintessence Publishing; 2008:123-164.
4. Gargiulo AW, Wentz F, Orban F. Dimensions and relations of the dentogingival junction in humans. J Periodontol. 1961;32:261-267.
5. Vacek JS: The dimensions of the human dentogingival junction. Int J Periodontics Restorative Dent. 1994;14(2):154-165.
6. Padbury A Jr, Eber R, Wang HL. Interactions between the gingiva and the margin of restorations. J Clin Periodontol. 2003;30(5):379-385.
7. Planciunas L, Puriene A, Mackeviciene G. Surgical lengthening of the clinical tooth crown. Stomatologija. 2006;8(3):88-95.
8. Goldberg PV, Higginbottom FL, Wilson TG. Periodontal considerations in restorative and implant therapy. Periodontol 2000. 2001;25:100-109.
9. Kokich VG. Adjunctive role of orthodontic therapy. In: Newman MG, Takei HH, Klokkevold PR, et al, eds. Clinical Periodontology. 10th ed. St Louis, MO: Elsevier; 2006:856-870.
10. Penny RE, Kraal JH. Crown-to-root ratio: its significance in restorative dentistry. J Prosthet Dent. 1979,42(1)34-38.
11. Tonetti MS, Claffey N. Advances in the progression of periodontitis and proposal of definitions of a periodontitis case and disease progression for use in risk factor research. Group C consensus report of the 5th European workshop in periodontology. J Clin Periodontol. 2005;32 (Suppl 6):210-213.
12. Renvert S, Persson GR. A systematic review on the use of residual probing depth, bleeding on probing and furcation status following initial periodontal therapy to predict further attachment and tooth loss. J Clin Periodontol. 2002;29 (Suppl 3):82-89.
13. Becker W, Becker BE, Berg LE. Periodontal treatment without maintenance. A retrospective study in 44 patients. J Periodontol.1984;
55(9):505-509.
14. Hill RW, Ramfjord SP, Morrison EC, et al. Four types of periodontal treatment compared over two years. J Periodontol. 1981;52(11):655-662.
15. Avila G, Galindo-Moreno P, Soehren S, et al. A novel decision-making process for tooth retention or extraction. J Periodontol. 2009;80(3):476-491.
16. Checci L, Montevecchi M, Gatto MR, et al. Retrospective study of tooth loss in 92 treated periodontal patients. J Clin Periodontol. 2002;29(7):651-656.
17. DeVore CH, Duckworth JE, Beck FM, et al. Bone loss following periodontal subjects without frequent periodontal maintenance. J Periodontol. 1986;57(6):354-359.
18. Hirschfeld L, Wasserman B. A long term survey of tooth loss in 600 treated periodontal patients. J Periodontol. 1978;49(5):225-237.
19. Lindhe J, Nyman S. The effect of plaque control and surgical pocket elimination on the establishment and maintenance of periodontal health. A longitudinal study of periodontal therapy in cases of advanced disease. J Clin Periodontol. 1975;2(2):67-79.
20. Lindhe J, Nyman S. Long-term maintenance of patients treated for advanced periodontal disease. J Clin Periodontal. 1984;11(8):504-514.
21. Cortellini P, Labriola A, Tonetti MS. Regenerative periodontal therapy in intrabony defects: state of the art. Minerva Stomatol. 2007;56(10):519-539.
22. Hamp SE, Nyman S, Lindhe J. Periodontal treatment of multirooted teeth. Results after 5 years. J Clin Periodontol. 1975;2(3):126-135.
23. Huynh-Ba G, Kuonen P, Hofer D, et al. The effect of periodontal therapy on the survival rate and incidence of complications of multirooted teeth with furcation involvement after an observation period of at least 5 years: a systematic review. J Clin Periodontol. 2009;36(2):164-176.
24. Needleman I. How long do multirooted teeth with furcation involvement survive with treatment? Evid Based Dent. 2010;11(2):38-39.
25. Murphy KG, Gunsolley JC. Guided tissue regeneration for the treatment of periodontal intrabony and furcation defects. A systematic review. Ann Periodontol. 2003;8(1):266-302.
26. Sculean A, Nikolidakis D, Schwarz F. Regeneration of periodontal tissues: combinations of barrier membranes and grafting materials - biological foundation and preclinical evidence: a systematic review. J Clin Periodontol. 2008;35(8 Suppl):106-116.
27. Jepsen S, Eberhard J, Herrera D, et al. A systematic review of guided tissue regeneration for periodontal furcation defects. What is the effect of guided tissue regeneration compared with surgical debridement in the treatment of furcation defects? J Clin Periodontol. 2002;29(Suppl 3):103-116.
28. Hovey LR, Jones AA, McGuire M, et al. Application of periodontal tissue engineering using enamel matrix derivative and human fibroblast-derived dermal substitute to stimulate periodontal wound healing in class III furcation defects. J Periodontol. 2006;77(5):790-799.
29. Palito DB, Joly JC, de Lima AF, et al. Clinical and radiographic treatment evaluation of class III furcation defects using GTR with and without inorganic bone matrix. J Clin Periodontol. 2003;30(1):1-8.
30. Johnson GK, Guthmiller JM. The impact of cigarette smoking on periodontal disease and treatment. Periodontol 2000. 2007;44:178-194.
31. Palmer RM, Wilson RF, Hasan AS, et al. Mechanisms of action and environmental factors—tobacco smoking. J Clin Periodontol. 2005;32(Suppl 6):180-195.
32. Johnson GK, Hill M. Cigarette smoking and the periodontal patient. J Periodontol. 2004;75(2):196-209.
33. Mattson JS, Cerutis DR. Diabetes mellitus: a review of the literature and dental implications. Compend Contin Educ Dent. 2001;22(9):757-764.
34. Farzaneh M, Abitbol S, Lawrence HP, et al. Treatment outcome in endodontics—the Toronto Study. Phase II: initial treatment. J Endod. 2004;30(5):302-309.
35. Naito T. Surgical or nonsurgical treatment for teeth with existing root filings? Evid Based Dent. 2010;11(2):54-55.
36. Sterrett JD, Oliver T, Robinson F, et al. Width/length ratios of normal crowns of the maxillary dentition in man. J Clin Periodontol. 1999;26(3):153-157.
37.Fradeani M. Esthetic rehabilitation in fixed prosthodontics: Esthetic analysis: A systemic approach to prosthetic treatment. Carol Stream, IL: Quintessence Publishing; 2004:250.
38. Kokich VO, Kokich VG, Kiyak HA. Perceptions of dental professionals and laypersons to altered dental esthetics: asymmetric and symmetric situations. Am J Orthod Dentofacial Orthop. 2006;130(2):141-151.