You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
By definition, local anesthesia causes a sensation loss in a specified area of the body caused by a depression of the excitation in nerve endings or an inhibition of the electrical action potential (impulses) that conducts along the nerve. Local anesthesia does not cause any loss of patient consciousness.1 Of the different theories on where local anesthesia works, the specific receptor theory is most favored. This theory states that the local anesthesia binds to the specific receptors on the sodium channel.2 By blocking the sodium channel, the nerves’ electrical action potential is not able to fire its impulse.
Local anesthestic solution is dispensed as salts commonly hydrochloride salt) that are dissolved in either sterile water or saline. This solution has a base (RN) and a cation (RNH+) (Figure 1). The two main factors that enable the local anesthesia to be effective are diffusion of the anesthetic through the nerve sheath and the binding of the drug at the receptor site.3
The uncharged, lipid-soluble, free base form (RN) diffuses through the nerve sheath. Once inside the sheath, a portion of the base (RN) reverts back into the cation form (RNH+) through a re-equilibration process. This occurs because the base (RN) cannot exist in the RN form at a pH of 7.4 (the normal pH of the interior of a nerve cell). Approximately 75% of the base is converted back to the cation (RNH+) inside the nerve sheath. It is the RNH+ cation that is then responsible for bonding to the sodium channel receptors and blocking the electric action potential of the nerve conduction pathway.3
The amount of base or cation available through the dissociation of the local anesthesia will have a direct effect on the ability for the local anesthetic solution to clinically achieve profound anesthesia for the patient. The dissociation of local anesthesia and the relative proportions of each form (cation and base), therefore, are dependent on the pH of the anesthetic solution and surrounding tissues. If a high pH (fewer H+ ions) exists, the chemical reaction is driven to the right (Figure 1), thus providing more base than cation to penetrate the nerve sheath. If a low pH (more H+ ions) exists, the chemical dissociation is driven to the left (Figure 1) and, therefore, more cation than base will be available and, hence, the local anesthetic solution will have more impedance in penetrating the nerve sheath.4
Objective Testing for Local Anesthesia Level
Prior to administering local anesthesia for endodontic treatment, the dentist needs to objectively test the treatment tooth with cold and/or an electric pulp tester (EPT). If the treatment tooth is non-responsive to preoperative objective tests, the adjacent tooth should be tested. With a preoperative baseline of the pulp vitality, once anesthesia is “onboard,” the level of anesthesia can be accessed by retesting the treatment tooth with cold or EPT. If the post-anesthesia tests are either negative to cold and/or an 80 EPT reading is obtained, the likelihood that the patient will be comfortable with the endodontic procedure is high. Nusstein et al5 define anesthetic success for mandibular anesthesia by achieving two consecutive EPT readings of 80 within 15 minutes and sustaining these reading for 60 minutes. It is important to note that in some cases of irreversible pulpitis, the treatment teeth can objectively test negative to cold or have an EPT reading of 80 and the patient still reports pain during treatment.6,7 It is these types of case scenarios in which supplemental anesthesia injections need to be administered.
Supplemental Local Anesthesia
Often, a patient will report “lip numbness” after an inferior alveolar nerve block or “cheek numbness” in a maxillary nerve block and the tooth to be endodontically treated will either test vital or not respond to vitality tests but still create discomfort upon endodontic tooth access. In order to obtain pulpal anesthesia in these patients, the clinician must administer supplemental local anesthesia.
Examples of supplemental local anesthesia injections are buccal nerve blocks (mandibular teeth), periodontal ligament (PDL), intraosseous, and intrapulpal. It is important to note that prior to administering any supplemental anesthesia, the dentist must first administer local anesthesia for a “regional” block. A “regional” block for the mandibular region is the inferior alveolar nerve block (IANB) and for maxillary teeth is the superior alveolar nerve block. If supplemental anesthesia is administered prior to a regional block, it will either be short-acting or not effective enough to provide pulpal anesthesia.
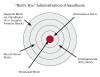
The goal in administering supplemental nerve blocks is to start systematically with a buccal nerve block in mandibular teeth and PDL block on maxillary teeth and progress the injection of anesthesia (as indicated) to an intrapulpal injection. An example of this graphically is the “bull’s eye” approach (Figure 2) from regional to intrapulpal anesthesia.8
The supplemental anesthesia clinical methodology is that after the anesthetic is injected into the buccal nerve for a mandibular tooth or the PDL of a maxillary tooth, the dentist should wait 3 to 5 minutes and then objectively test the treatment tooth with cold and/or EPT. If the mandibular or maxillary treatment tooth test non-responsive, the dentist should proceed with the endodontic treatment. If the patient, for whatever reason, still reports di comfort upon access into the pulp chamber, an intrapulpal injection should be administered. When administering a mental nerve block (buccal block for the lower anterior teeth), the dentist should have their patient apply hand pressure extraorally over the site of the mental nerve until he or she feels the further onset of the local anesthetic. This clinical technique will significantly reduce the onset time of the anesthesia to take effect.
If the mandibular tooth still tests vital in the above case scenario, a PDL injection should then be administered. The reason for this is a study by Matthews et al9 that reported a 58% success rate for buccal infiltration on patients diagnosed with irreversible pulpitis. If the maxillary treatment tooth still tests vital, a second PDL injection should be administered. A study by Cohen et al10 demonstrated that a reinjection of the PDL increased the success rate from 74% to 96% on teeth with a pretreatment pulpal diagnosis of irreversible pulpitis. It is important to note that the local anesthesia delivered from a PDL injection reaches the pulp through the penetration of the cancellous bone through the natural osseous perforations in the tooth socket.11 The success of a PDL injection depends on the dentist’s ability to create back-pressure during the injection.5
If a PDL injection in conjunction with the regional block and buccal nerve block in the case with a mandibular tooth does not achieve pulpal anesthesia, an intraosseous block should be considered. To a clinician who has never administered an intraosseous local anesthetic injection before, it may seem a challenging task. But, with a didactic understanding and some clinical practice on easier cases, the dentist will find the intraosseous injection a valuable part of his or her local anesthesia technique. The three main intraosseous injection systems available on the market are Stabident™ (Fairfax Dental, Inc.), X-Tip™ (DENTSPLY Tulsa, www.tulsa.com), and IntraFlow™ (DenTrek, www.dentrek.com). Although each system varies slightly on specific clinical usage, the main similarities are that they all should be given distal to the tooth to be anesthetized, the anesthetic solution should be placed directly into the cancellous bone surrounding the treatment tooth, and an immediate onset of local anesthesia after solution placement will be achieved.5
It is not u common that even after administering supplemental local anesthesia to a patient that although the treatment tooth tests negative to cold and/or EPT, the administration of an intrapulpal injection will be necessary. Intrapulpal anesthesia is achieved as a result of pressure and not from the actual type of anesthesia.11
When performing an intrapulpal injection, a small cavity should be created in the pulp chamber and the anesthetic needle should fit “snugly” into the access that was created. This will allow the anesthetic solution to be delivered under pressure. You should advise the patient that there may be a slight di comfort during this procedure, but the anesthesia will have a rapid onset and the patient will become comfortable with the initiation of endodontic treatment.12
In the event that a small access cavity into the pulp chamber cannot be created due to clinical factors such as extensive decay, local anesthesia should be placed on the exposed pulp for about a minute before advancing the needle as far apically as possible into pulp chamber in order to inject the anesthetic solution under pressure.12
There will be cases when the clinician is able to access the pulp chamber and initiate file placement in the canal, but the patient still reports di comfort when the file advances in the apical one third of the canal. Unfortunately, local anesthesia needles are too large to place anesthetic solution in this area. An alternative anesthesia technique is to place topical anesthetic on a #10 or #15 hand file and then advance the file into the apical one third of the canal to effectively anesthetize and remove the vital pulp fragments. When using this technique, a very slight amount of topical anesthetic should be applied to the hand file. Too much topical anesthetic can coat the canal walls and affect the sealing of the canal during obturation. Also, when the topical anesthetic mixes with the sodium hypochlorite, it can create a darkish red color and can be mistaken for blood.13
In conjunction with the integration of regional and supplemental local anesthesia techniques, the selection of the correct type of local anesthesia will also play an important role in improving consistency and efficiency in obtaining profound pulpal anesthesia.
Choosing the CorrectLocal Anesthetic
Regional Block
Dental schools have a history of teaching that the more a local anesthetic containing a vasoconstrictor (ie, epinephrine) is administered, the faster and more profound the local anesthetic effects will be for the patient. However, this methodology for administering an anesthetic with only a vasoconstrictor can actually delay the uptake of anesthetic in patients.8
Epinephrine is acidic and, therefore, lowers the pH of the injection site. This lowered pH (as stated above) will enable fewer amounts of base (RN) to be available for nerve-sheath penetration. Also, although epinephrine acts on both alpha receptors (vasoconstriction) and beta receptors (vasodilatation, bronchodilation, and increasing heart rate and contraction) its effects on beta receptors is equal to its effect on alpha receptors.14 This will affect the amount of vasoconstriction that will actually occur in the injection site.
When giving a regional block—either an IANB or superior alveolar block—the dentist should administer one carpule of an anesthetic with a vasoconstrictor and then wait a few minutes to observe if the patient reports any subjective signs (ie, feeling numb or feeling like the lip or cheek is “fat”). If the patient states that they feel the anesthetic is taking effect, the clinician did not miss the anatomical block and should proceed with an anesthetic with no vasoconstrictor. If the patient does not report any subjective findings in regards to “feeling numb,” this is a sign that either the anatomical block was missed or there is not enough concentration of base “onboard” to penetrate the nerve sheath. Either way, the second carpule of anesthesia should still be 3% mepivicaine with no epinephrine. After administering this second carpule of anesthetic, if the patient begins to feel numb, it was anesthetic concentration and, if not, one needs to re-evaluate the anatomical placement of the anesthetic.
Clinically, the use of levonordefrin as a replacement for epinephrine will produce less cardiac and central nervous system stimulation. A study by Lawaty et al15 demonstrated that there was no significant difference in anesthetic success between 2% mepivacaine with 1:20,000 levonordefrin and 2% lidocaine with 1:100,000 epinephrine. Levonordefrin acts 75% on alpha receptors and 25% on beta receptors.14
Since the introduction of articaine into the US market, studies have demonstrated that there is no significant difference between 4% articaine with 1:100,000epinephrine and 2% lidociane with 1:100,000 epinephrine in IANB anesthesia.16,17 It is important to note that studies have reported a higher incidence of paresthesia when articaine has been administered for IANB. Although the exact etiology of the paresthesia is unknown, it is hypothesized that the neurotoxicity may be due to the higher concentration of local anesthesia used: 4% articaine as compared to 2% lidocaine.18,19 The clinician must consider these risks to the benefits of administering 4% articaine for IANB anesthesia.
Buccal Block
When administering anesthesia for a buccal block, the use of 4% articaine with 100,000 epinephrine should be the drug of choice.18 A study by Srinivasan et al20 reported that the efficacy of 4% articaine with 100,000 epinephrine was superior to 2% lidocaine with 100,000 epinephrine for buccal infiltrations in maxillary posterior teeth.
Periodontal Ligament Block
The use of 2% lidocaine with 100,000 epinephrine has been demonstrated to be significantly better in achieving pulpal anesthesia through a PDL injection as compared to using a local anesthetic without a vasoconstrictor.11,21
Intraosseous Block
Although the literature supports the use of an anesthetic with a vasoconstrictor for administering for an intraosseous block,22 the clinician needs to be aware that this will increase most patients’ heart rate.23 Therefore, a clinician needs to balance a longer anesthetic effect along with a tachycardia response of the patient as compared to using 3% mepivacaine (with no epinephrine) and eliminating the cardiac effect, but shortening the duration of the local anesthetic effect. A study by Reisman et al24 reported that when a repeated intraosseous injection with 3% mepivacaine (with no epinephrine) was administered, there was an increase in anesthetic success to 98%. Emperically, most patients get an uncomfortable feeling when their heart begins to race after the epinephrine enters their system systemically as the result of the intraosseous block.
Intrapulpal Block
As stated previously, the main objective in administering an intrapulpal anesthesia is to give it under pressure. Although it has been stated in the literature that saline is as effective as 2% lidocaine with 1:100,000 epinephrine in providing anesthesia intrapulpally,25,26 it is r.commended to use 2% lidocaine with 1:00,000 epinephrine. Emperically, the use of anesthetic with a vasoconstrictor will provide some vasoconstriction on the pulpal vascular system. This is important because most pulps with irreversible pulpitis can be hyperemic because of the body’s attempt to address the localized inflammation.
Conclusion
It is paramount that dentists recognize local anesthesia as a drug. Understanding how local anesthesia works in conjunction with conducting proper objective testing for anesthesia levels, administering supplemental anesthesia, and selecting the correct type of local anesthesia will allow clinicians to enhance their consistency and efficiency in obtaining profound pulpal anesthesia on their endodontic patients.
Disclosure
Dr. James Bahcall has no financial interest in any of the products mentioned in this article and received no compensation for writing this article.
References
1. Malamed SF. Handbook of Local Anesthesia. 5th ed. St. Louis, MO: Elsevier Mosby; 2004:3.
2. Berry CA, Sanner JH, Keasling HH. A comparison of the anticonvulsant activity of mepivacaine and lidocaine. J Pharmacol Exp Ther. 1961;133:357-363.
3. Malamed SF. Handbook of Local Anesthesia. 5th ed. St. Louis, MO: Elsevier Mosby; 2004:16-24.
4. Malamed SF. Handbook of Local Anesthesia. 4th ed. St. Louis, MO: Elsevier Mosby; 1997:14-17.
5. Nusstein J, Reader A, Drum M. Local anesthesia strategies for the patient with a “hot” tooth. Dent Clin N Am. 2010;54(2):237-247.
6. Dreven LJ, Reader A, Beck M, et al. An evaluation of an electric pulp tester as a measure of analgesia in human vital teeth. J Endod. 1987;13(5):233-238.
7. Hsiao-Wu GW, Susaria SM, White RR. Use of the cold test as a measure of pulpal anesthesia during endodontic therapy: a randomized, blinded, placebo-controlled clinical trial. J Endod. 2007;33(4):406-410.
8. Bahcall J. Everything I know about endodontics, I learned after dental school. Dent Today. 2003;22:84-86.
9. Matthews R, Drum M, Reader A, et al. Articaine for supplemental buccal mandibular infiltration anesthesia in patients with irreversible pulpitis when the inferior alveolar nerve block fails. J Endod. 2009;35(3):343-346.
10. Cohen H, Cha B, Spangberg L. Endodontic anesthesia in mandibular molars: a clinical study. J Endod. 1993;19(7):370-373.
11. Meechan JG. Supplementary routes to local anesthesia. Int Endod J. 2002;35(11):885-896.
12. Meechan JG. How to ove come failed local anesthesia. Br Dent J. 1999;186(1):15-20.
13. DeNunzio M. Topical anesthetic as an adjunct to local anesthesia during pulpectomies. J Endod. 1998;24(3):202-203.
14. Malamed SF. Handbook of Local Anesthesia. 5th ed. St. Louis, MO: Elsevier Mosby; 2004:45-49.
15. Lawaty I, Drum M, Reader A, Nusstein J. A prospective, randomized, double-blind comparison of 2% mepivacaine with 1:20,000 levonordefrin versus 2% lidocaine with 1;100,000 epinephrine for maxillary infiltrations. Anesth Prog. 2010;57(4):139-144.
16. Brandt R, Anderson P, McDonald N, et al. The pulpal anesthetic efficacy of articaine versus lidocaine in dentistry: A meta-analysis. J Am Dent Assoc. 2011;142(5):493-504.
17. Mikeseil P, Nusstein J, Reader A, et al. A comparison of articaine and lidocaine for inferior alveolar nerve blocks. J Endod. 2005;31(4):265-270.
18. Haas DA, Lennon D. A 21 year retrospective study of reports of paresthesia following local anesthetic administration. J Can Dent Assoc. 1995;61(4):319-330.
19. Garisto G, Gaffen A, Lawrence H, et al. Occurrence of paresthesia after dental local anesthetic administration in the United States. J Am Dent Assoc. 2010;141(8):836-844.
20. Srinivasan N, Kavitha M, Loganathan C, Padmini G. Comparison of anesthetic efficacy of 4% articaine and 2% lidocaine for maxillary buccal infiltration in patients with irreversible pulpitis. Oral Surg Oral Med Oral Pathol Oral Radio Endod. 2009;107(1):133-136.
21. Gray RJ, Lomax AM, Rood JP. Periodontal ligament injection: with or without a vasoconstrictor? Br Dent J. 1987;162(7):263-265.
22. Repogle K, Reader A, Nist R, et al. Anesthetic efficacy of the intraosseous injection of 2% lidocaine (1:100,000 epinephrine) and 3% mepivacaine in mandibular first molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;83(1):30-37.
23. Coggins R, Reader A, Nist R, et al. Anesthetic efficacy of the intraosseous injection in maxillary and mandibular teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996;81(6):634-641.
24. Reisman D, Reader A, Nist R, et al. Anesthetic efficacy of the supplemental intraosseous injection of 3% mepivacaine in irreversible pulpitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84(6):676-682.
25. Malamed SF. The management of pain and anxiety. In: Cohen S, Burns RC, eds. Pathways of the Pulp. 7th ed. St. Louis, MO: Elsevier Mosby; 1998:665-666.
26. Van Gheluwe MS, Walton R. Intrapulpal injection. Factors related to effectiveness. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;83(1):38-40.
For product information on Local Anesthesia, visit: dentalaegis.com/go/id212
For additional content on Local Anesthesia, visit: dentalaegis.com/go/id213
About the Author
James Bahcall, DMD, MS
Associate Professor
College of Dental Medicine
Midwestern University
Downers Grove, Illinois